
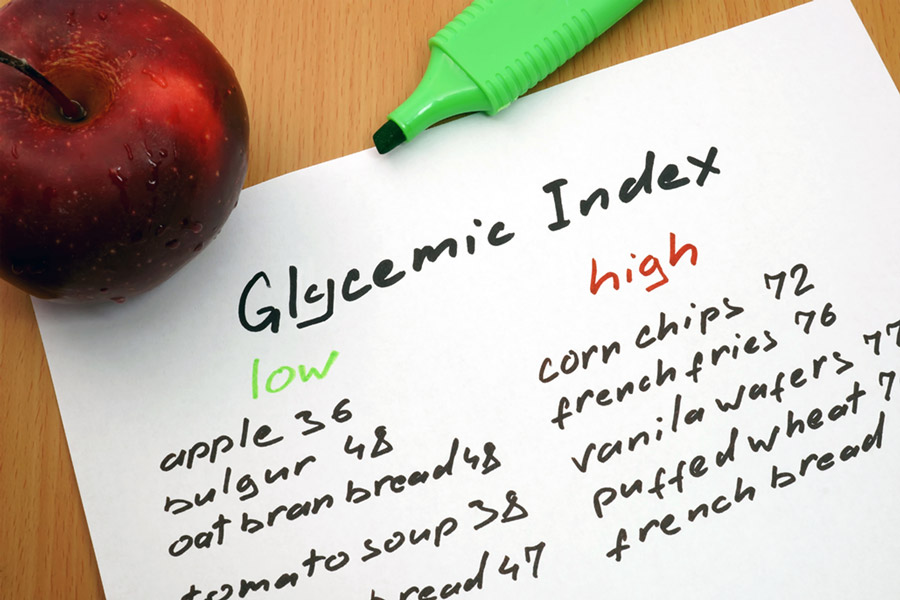
A term commonly used in nutrition discussions about diet is glycemic index. Glycemic index is formally defined as the amount that a food consumed by itself by someone in a fasting state will raise that person’s blood glucose level over a two-hour period of time relative to a reference carbohydrate consumed under the same conditions. Higher glycemic index foods are simple sugars and highly refined grains because they are quick to digest, pass thru the stomach, and be absorbed into the blood stream from the intestines.
It is generally considered advantageous to health to avoid eating large amounts of simple sugars and refined carbohydrates. An important reason for this is that, except during vigorous physical exertion, the sudden spike in blood glucose levels that results from high glycemic index foods can lead to an exaggerated rise in insulin levels. This in turn raises serum triglyceride levels and low-density lipoproteins (the so-called bad cholesterols). Both of these lipids are associated with increased disease risks. Additionally, the spike in serum glucose has been associated with increased vascular and organ inflammatory mediators which are thought to contribute to development of atherosclerosis and multiple different organ diseases.
Nearly all studies looking at our dietary patterns over the last several decades have reached the same conclusion: Americans obtain too many of their calories from processed and refined carbohydrate sources, the so-called “bad carbohydrates.” Restricting these makes sense in any diet for weight loss or health promotion. When other calories are not consumed in the place of these eliminated food sources, then, by definition, the individuals who are restricting these carbohydrate sources will be achieving a negative energy balance and will lose weight. This is important to understand: the stored energy (fat mass) loss that comes from a carbohydrate restriction diet comes from a reduction in total energy intake so the only way to lose fat mass is to consume fewer calories than you burn. It just so happens that excess high glycemic index foods are a convenient way to do this because they are almost always over-consumed by overweight and obese individuals.
A common observation from patients when they implement a carbohydrate restriction diet is that they experience rapid weight loss. This is indeed often the case since simple sugars are most often the main source of excess calories in the American diet. Unfortunately, the rapid loss of large amounts of weight, out of proportion to the actual caloric restriction, that patients often report is not caused by fat loss (what one wants) but by excretion of large amounts of water that ordinarily is bound to stored glycogen. This water weight loss will re-equilibrate over time, and, in point of fact, carbohydrate-restriction diets have never been shown to be superior to other calorie restricting diets for long-term weight loss. Therefore, I tell patients that trying to avoid all carbohydrates so they can lose weight is not a productive long-term strategy and misses the most important point that there is a significant difference among the types and sources of carbohydrates. They should restrict high glycemic index carbohydrates, but fruits, vegetables, and whole grains are not intrinsically concerning, and should, in reality, continue as important energy sources. Individuals should consume health-promoting whole food carbohydrate sources and avoid the “bad carbohydrates” such as those high in added simple sugars, added high fructose corn syrup, and highly refined grains which all have a high glycemic index.
By Dr. Eric Zacharias
References:
- Dietary Guidelines for Americans Committee; U.S. Department of Agriculture. Center for Nutrition Policy and Promotion. Dietary guidelines for Americans, 2010. Accessed 19 July 2024.
- Daniels SR, Jacobson MS, McCrindle BW, Eckel RH, Sanner BM. American Heart Association Childhood Obesity Research Summit: executive summary. Circulation. 2009;119(15):2114-23.
- Gilliland FD, Berhane K, Islam T, McConnell R, Gauderman WJ, Gilliland SS, Avol E, Peters JM. Obesity and the risk of newly diagnosed asthma in school-age children. Am J Epidemiol 2003;158(5):406-15.
- Pi-Sunyer X. The medical risks of obesity. Postgrad Med. 2009;121(6):21-33.
- Rofey, DL, Kolko RP, Iosif, AM, Silk JS, Cost JE, Feng W, et. al. A longitudinal study of childhood depression and anxiety in relation to weight gain. Child Psychiatry Hum Dev, 2009;40(4):517-26.
- Centers for Disease Control. National Center for Health Statistics (NCHS). http://www.cdc.gov/nchs/. Accessed 27 May 2011.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303(3):235-41.
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA, 2010;303(3):242-9.
- Ogden CL, Carroll MD, Flegal KM. High body mass index for age among US children and adolescents, 2003-2006. JAMA. 2008;299(20):2401-5.
- US Department of Health and Human Services. The Surgeon General’s call to action to prevent overweight and obesity: overweight in children and adolescents. Washington, DC: US Department of Health and Human Services; 2007.
- Singh AS, Mulder C. Twisk JW, van Mechelen W, Chinapaw MJ. Tracking of childhood overweight into adulthood: a systematic review of the literature. Oces Rev. 2008;9(5):474-88.
- Mission: Readiness- Military Leaders for Kids. Too fat to fight retired military leaders want junk food out of America’s schools. New York: Mission Readiness; 2010.
- Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH. Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med. 1992;327(19):1350-5.
- Latner, JD, Stunkard AJ, Wilson GT. Stigmatized students: age, sex, and ethnicity effects in the stigmatization of obesity. Obes, Res, 2005;13(7): 1226-31.
- Wang Y, Beydoun MA, Liang L, Caballero B, Kumanyika SK. Will all Americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity (Silver Spring). 2008;16(10):2323-30.
- Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff (Millwood). 2009;28(5):w822-31.
- Nielson SJ, Popkin BM. Patterns and trends in food portion sizes, 1977-1998. JAMA. 2003;289(4):450-3.
- Mellen PB, Gao SK, Vitolins MZ, Goff Jr DC. Deteriorating dietary habits among adults with hypertension: DASH dietary accordance, NHANES 1988-1994 and 1999-2004. Arch Intern Med, 2008;168(3):308-14.
- Ello-Martin JA, Ledikwe JH, Rolls BJ. The influence of food portion size and energy density on energy intake: implications for weight management. Am J Clin Nutr. 2005;82(1 Suppl):236S-41.
- Fisher, JO, Kral, TV. Super-size me: portion size effects on young children’s eating, Physiol Behav. 2008;94(1):39-47.
- Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr. 2006;84(2)274-88.
- Sichieri R, Paula Trotte A, de Souza RA, Veiga GV. School randomized trial on prevention of excessive weight gain by discouraging students from drinking sodas. Public Health Nutr. 2009;12(2):197-202.
- Bowman SA, Vinyard BT. Fast food consumption of U.S. adults: impact on energy and nutrient intakes and overweight status. J Am Coll Nutr. 2004;23(2):163-8.
- Kant AK, Graubard BI. Eating out in America, 1987-2000: trends and nutritional correlates. Prev Med. 2004;38(2):243-9.
- Rosenheck R. Fast food consumption and increased caloric intake: a systematic review of a trajectory towards weight gain and obesity risk. Obes Rev. 2008;9(6):535-47.
- Gilhooly CH, Das SK, Golden JK, McCrory MA, Dallal GE, Saltzman E, Kramer FM, Roberts SB. Food cravings and energy regulation: the characteristics of craved foods and energy regulation: the characteristics of craved foods and their relationship with eating behaviors and weight change during 6 months of dietary energy restriction. Int J Obes (Lond). 2007;31(12):1849-58
- Hannum Sm, Carson LA, Evans EM, Petr EL, Wharton CM, Bui L, Erdman Jr JW. Use of packaged entrees as part of a weight-loss diet in overweight men: an 8-week randomized clinical trial. Diabetes Obes Metab. 2006;8(2):146-55.
- Pearcey SM, de Castro JM. Food intake and meal patterns of weight-stable and weight-gaining persons. Am J Clin Nutr. 2002;76(1):107-12.
- Rolls BJ, Morris EL, Roe LS. Portion size of food affects energy intake in normal-weight and overweight men and women. Am J Clin Nutr. 2002;76(6):1207-13.
- Rolls BJ, Roe LS, Kral TV, Meengs JS, Wall DE. Increasing the portion size of a packaged snack increase energy intake in men and women. Appetite. 2004;42(1):63-9.